

Severe asthma in adults and adolescents is uncommon, but important to recognize early because delaying diagnosis also delays effective treatment. Read on to find out more about what the symptoms of severe asthma in adults and adolescents are, why it happens and how it can be diagnosed.
Managing severe asthma is often a team effort between the person with asthma, their GP, the practice nurse and specialist doctors such as lung physicians and allergists. Monoclonal antibody treatment can be very effective for severe asthma and is available in Australia under the PBS with a specialist prescription.
Casey’s story
“My doctor told me I was already on the highest dose preventer medication for my asthma that she could describe and that I would need to see a lung specialist. I was disappointed because we had worked so hard to address all my asthma triggers.
I had quit smoking a few years ago, and even gotten my weight under control. I had changed my diet so I wasn’t getting reflux anymore. My GP told me my inhaler technique was perfect and I had been using my preventer every day. Despite all this my asthma symptoms continued; I kept coughing and felt short of breath. I was tired of taking days off and always having to see the doctor.
I thought that I might not even have asthma, because my medications started to feel like they weren’t working well enough. When I finally saw the lung specialist he did all these tests to confirm that not only did I have asthma, but that it was severe asthma.
Thankfully, because we were able to confirm this, I was started on a new add-on medication - but as an injection. My asthma control became so much better after this.”
What is Severe Asthma?
Generally, asthma is severe when symptoms are hard to control despite properly using high dose steroid medications for asthma, either inhaled (in combination with a long acting beta agonist) or taken orally.
More specifically, a doctor will check the following before diagnosing severe asthma:
-
There are asthma symptoms and your doctor has ruled out other medical conditions that can causes these symptoms
-
The asthma symptoms continue despite:
-
high doses of standard asthma preventer medication (inhaled corticosteroid + long acting beta agonist), using their medication regularly and using good inhaler technique
-
Avoiding exposure to asthma triggers where possible, and addressing other medical conditions that can worsen asthma (such as reflux or hayfever)
How Common is Severe Asthma?
Severe asthma is uncommon, affecting less than 4% (1 in 25) of people with asthma.

Fig 1. Prevalence of severe asthma. Around 1 in 9 (green) Australians live with asthma, but of these only 1 in 25 (orange) will have true severe asthma.
Severe Asthma vs. Uncontrolled Asthma: What's the Difference?
You might have heard the terms “uncontrolled asthma” or “difficult-to control asthma”. Importantly, these are not the same as “severe asthma”.
In many people with asthma, symptoms are uncontrolled because:
-
Prescribed asthma medications are not being used regularly
-
Inhaler technique is not very good
-
Avoidable triggers for asthma are not being addressed (such as hay fever)
Your GP can help you with optimizing your medication and managing triggers. In severe asthma, symptoms continue despite doing all of the above.
Severe Asthma vs. Severe Asthma Attack: What’s the Difference?
“Severe asthma” is not the same as a “severe asthma attack”.
“Severe asthma” refers to how asthma is controlled in the long term.
On the other hand, a “severe asthma attack” is a medical emergency, needing immediate treatment as guided by the person’s asthma action plan, and if necessary calling an ambulance or seeking urgent medical assistance.
Click here to learn more about severe asthma attacks.
What Are the Symptoms of Severe Asthma?
The symptoms of severe asthma are the same as other forms of asthma. The difference is that they are much harder to control despite high dose inhaled corticosteroid + long acting beta agonist medication. Click here to learn more about asthma symptoms.
What Causes Severe Asthma?
The reasons why people get severe asthma are complex, but the short answer is that people with severe asthma have differences in how their immune system works in response to triggers causing more inflammation.
This inflammation then causes changes to how your lungs and airways work:
-
Your airways become more sensitive or “hyperresponsive”
-
The muscles around your airways get bigger (not in a good way!)
-
Airway muscles squeeze the airways too tightly (bronchoconstriction)
-
Your lungs produce too much mucus
-
Excess collagen (like scar tissue) in the airways makes them too stiff
Inflammation is an important way for your immune system to fight off infections. Scientists have worked out that different types of inflammation can occur in asthma. Depending on the type of inflammation, we might see abnormally high levels of immune cells driving the asthma. Understanding which type of inflammation is at play can help your doctor work out your asthma phenotype.
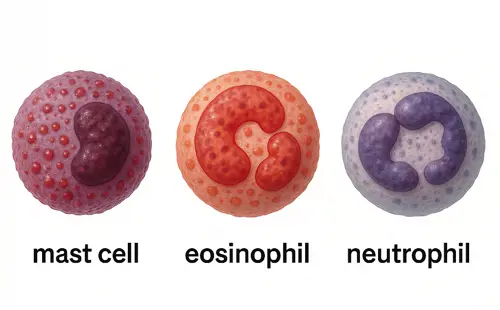
Figure 2. Mast cells and Eosinophils are seen in asthma driven mainly by Type 2 inflammation. Neutrophils are activated by non-type 2 inflammation. These cells cause changes in the lungs and airways resulting in asthma symptoms.
Type 2 inflammation activates eosinophils, and is an important way for the body to fight infection. But in many people with asthma it can become overactive after exposure to allergens, such as dust, pollens or pet fur. Examples of causes of persisting type 2 inflammation could include:
-
Allergic bronchopulmonary aspergillosis
-
Aspirin exacerbated respiratory disease
-
Continued allergen exposure at home and at work
Viruses that cause coughs and colds naturally activate non-type 2 inflammation, increasing neutrophils in the airway. Other examples causing this include:
-
Sinusitis
-
Bacterial infections
-
Smoke or pollutant inhalation
Severe asthma that is driven by type 2 inflammation with eosinophils is probably most common, but non-type 2 inflammation with neutrophils is also present in a lot of people with severe asthma. Less often people might have a mix of both.
It is also possible to have severe asthma without much evidence of any inflammation at all (paucigranulocytic asthma). This may be due to the long term changes to the structure of the lungs and airways that persist after inflammation has settled. It may also highlight differences to how the lungs respond to the nerves and hormones that control it.
How is Severe Asthma Diagnosed?
First, your doctor needs to confirm that your symptoms are indeed from asthma and not something else. Part of this will be identifying avoidable triggers where possible, and managing other conditions that may be worsening asthma, such as reflux or hay fever.
Second, your asthma is diagnosed as severe if symptoms continue or are difficult to control despite regularly and properly using high doses of a standard preventer (combined inhaled-corticosteroid + long acting beta agonist medication).
Third, your doctor may refer you to a specialist who can help work out what your asthma phenotype is.
Diagnosing severe asthma is complex and will usually take a few visits, with your doctor, asking you questions about your health, examining you, and checking on your medications. Your GP might recommend testing such as:
-
chest x-rays
More sophisticated tests are usually overseen by a specialist, but can include:
-
Blood tests to measure neutrophils, eosinophils or IgE antibodies
-
Sputum (phlegm) testing to measure neutrophils or eosinophils
-
Fractional exhaled nitric oxide (FeNO) level
-
CT scans of your chest
-
Allergy testing (skin prick or blood testing)
-
Bronchial challenge testing
Understanding Asthma Phenotypes
Phenotype means “the visible traits or properties” of something. So understanding your asthma phenotype means working out what traits we can observe about it. Your doctor may check eosinophil or neutrophil levels:
-
Severe Asthma with Eosinophilic airway inflammation – higher levels of eosinophils are seen in the blood and sputum
-
Severe Asthma with Neutrophilic Airway Inflammation – more neutrophils are observed in the sputum
-
Mixed Eosinophilic and Neutrophilic Airway Inflammation - properties of both are seen
-
Paucigranulocytic (Noninflammatory) Asthma - neither properties of both are seen
Your doctor may also recommend Spirometry [link to spirometry article] or bronchial challenge testing to further define the severe asthma phenotype:
-
Hyperresponsive and Variable Obstruction - the airways constrict and narrow easily in response to certain triggers, but can still have a good response to asthma relievers
-
Fixed Obstruction - the airways have difficulty getting air out with or without triggers, and have a limited response to asthma relievers
What Are the Treatment Options for Severe Asthma?
Unless instructed by a doctor, important aspects of severe asthma treatment are:
-
Preventer medication: regular high dose inhaled corticosteroid medication (in combination with a long acting beta agonist)
-
Reliever medication which is available at all times
-
Optimizing inhaler technique
-
A current asthma action plan
-
Management of other medical conditions and triggers known to worsen asthma
-
Treating any current respiratory infections
-
Preventing respiratory infections by ensuring immunizations are up to date
Some people find switching to a maintenance and reliever therapy (MART) regimen improves their asthma control, but this should be discussed with a doctor first.
If severe asthma remains uncontrolled with a high dose inhaled corticosteroid (combined with a long acting beta agonist), add-on treatments might be tried and must be guided by your doctor. Examples include:
-
Long-acting muscarinic agonists (such as Tiotropium, Glycopyrronium, Umeclidinium)
-
Montelukast
Depending on the case, specialists may also consider add-on treatments such as:
-
Monoclonal antibody therapy (also known as “biologics”)
-
Long term low dose antibiotics known as macrolides
-
Longer courses of oral corticosteroids
Lastly, bronchial thermoplasty is a specialist medical procedure whereby heat is directed into the airways to wear away the muscles that cause constriction and narrowing. This treatment is currently being investigated for severe asthma, and should only be considered after being seen in a highly specialised severe asthma clinic.
Treatments based on Severe Asthma Phenotype
Deciding treatment based on severe asthma phenotype must be guided by a specialist doctor such as a respiratory physician or allergist/immunologist.
In severe asthma with eosinophilic airway inflammation (or type 2 inflammation) or even mixed inflammation, then monoclonal antibody therapies may be an effective option, as these medicines target the processes that cause type 2 inflammation. These are available as injections given under the skin, and include:
-
Benralizumab (Fasenra)
-
Dupilumab (Dupixent)
-
Mepolizumab (Nucala)
-
Omalizumab (Xolair)
In Australia, monoclonal antibody therapy for treating severe asthma can be subsidized by the PBS, provided that the person with severe asthma has been under the care of the specialist for at least 6 months. As a result, it is important not to delay seeing a specialist if severe asthma is suspected.
What Natural Treatments Can Help?
Some people with severe asthma can benefit from practicing a technique used by physiotherapists called “active cycle of breathing”, particularly if excessive mucus is a problem.
Your GP might suggest referral to a physiotherapist as part of your asthma care plan.
Do Lifestyle Changes Make a Difference?
A healthy diet and lifestyle play a crucial role in managing severe asthma. Avoiding asthma triggers and quitting smoking is a must if you have severe asthma.
Regular exercise and keeping a healthy weight helps improve lung capacity and overall health, but always check with your doctor before starting a new routine.
Stress can trigger asthma symptoms, so managing it effectively is important. Techniques such as deep breathing, yoga, meditation, and progressive muscle relaxation can help reduce stress and improve well-being.
By maintaining a balanced diet, staying active, and managing stress, you can better control severe asthma symptoms and improve your quality of life.
Managing and Preventing Severe Asthma
It is not always possible to prevent severe asthma from developing, but it can be identified early so optimal management can be put in place.
Correct diagnosis
-
Other medical conditions can look like severe asthma, and severe asthma can also co-exist with other medical conditions
-
See your GP to ensure that are symptoms are indeed from asthma, and that there are no other medical conditions contributing to the asthma
-
Spirometry is a key investigation for diagnosing and monitoring asthma
Proper Use of Inhaler Medication
-
Severe asthma can only be diagnosed if asthma symptoms continue despite proper and regular use of a high dose inhaled corticosteroid (combined with long acting beta agonist) medication
-
Always use your asthma medications as prescribed. If you feel the prescription is not working for you, then see your GP as soon as possible.
-
Correct technique is key to effective asthma control. See your GP or practice nurse to ensure your inhaler technique is optimal.
Asthma Action Plan
-
Developed with your GP or specialist, this plan outlines daily medication, how to handle flare-ups, triggers to avoid, and when to seek help. Click here to learn more.
Regular Follow-ups with your GP
-
Ask your GP about a chronic disease management plan for severe asthma
-
Routine check-ups (every 3-6 months) are essential to monitor symptoms, adjust medications, and prevent complications
-
Ensure your immunizations are up to date
Early referral to a specialist or multi-disciplinary severe asthma team
-
Ask your GP about a referral to a specialist if you suspect you have severe asthma
-
Delaying specialist referral for severe asthma can also mean delaying effective treatment, such as monoclonal antibody therapy
Useful Resources
-
Australian Bureau of Statistics. (2022). Asthma, 2022. Retrieved from https://www.abs.gov.au/statistics/health/health-conditions-and-risks/asthma/latest-release
-
National Asthma Council Australia. (n.d.). Australian Asthma Handbook. Retrieved from https://www.nationalasthma.org.au/health-professionals/australian-asthma-handbook
-
Centre of Excellence in Severe Asthma. (n.d.). Prevalence & Burden. Retrieved from https://toolkit.severeasthma.org.au/severe-asthma/prevalence-burden/
-
National Asthma Council Australia. (2023). Heat maps identify asthma “hot spots” in WA, NT and Tas. Retrieved from https://www.nationalasthma.org.au/news/2023/heat-maps-identify-asthma-hot-spots-in-wa-nt-and-tas
-
Australian Institute of Health and Welfare. (n.d.). Asthma. Retrieved from https://www.aihw.gov.au/reports/chronic-respiratory-conditions/asthma
-
National Institute of Allergy and Infectious Diseases (NIAID). (n.d.). Asthma. Retrieved February 27, 2025, from https://www.niaid.nih.gov/diseases-conditions/asthma
-
Asthma & Allergy Foundation of America. (n.d.). Asthma. Retrieved February 27, 2025, from https://aafa.org/asthma/
References
-
Israel E, Reddel HK. Severe and Difficult-to-Treat Asthma in Adults. N Engl J Med. 2017 Sep 7;377(10):965-976. doi: 10.1056/NEJMra1608969. PMID: 28877019.
-
National Asthma Council Australia. (n.d.). Australian Asthma Handbook. Retrieved from https://www.nationalasthma.org.au/health-professionals/australian-asthma-handbook
-
Hains I, Meyers J, Sterling K, Yoo J, Reddel H, Weston C. Difficult-to-treat and severe asthma in general practice: delivery and evaluation of an educational program. BMC Fam Pract. 2019 Jul 13;20(1):99. doi: 10.1186/s12875-019-0991-y. PMID: 31301742; PMCID: PMC6626400.
-
Holguin F, Cardet JC, Chung KF, Diver S, Ferreira DS, Fitzpatrick A, Gaga M, Kellermeyer L, Khurana S, Knight S, McDonald VM, Morgan RL, Ortega VE, Rigau D, Subbarao P, Tonia T, Adcock IM, Bleecker ER, Brightling C, Boulet LP, Cabana M, Castro M, Chanez P, Custovic A, Djukanovic R, Frey U, Frankemölle B, Gibson P, Hamerlijnck D, Jarjour N, Konno S, Shen H, Vitary C, Bush A. Management of severe asthma: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2020 Jan 2;55(1):1900588. doi: 10.1183/13993003.00588-2019. PMID: 31558662.
-
Schoettler N, Strek ME. Recent Advances in Severe Asthma: From Phenotypes to Personalized Medicine. Chest. 2020 Mar;157(3):516-528. doi: 10.1016/j.chest.2019.10.009. Epub 2019 Oct 31. PMID: 31678077; PMCID: PMC7609962.
-
Quint JK, Shah PL. What trials do and do not tell us about treatments for severe asthma. Lancet. 2024 Jan 20;403(10423):224-226. doi: 10.1016/S0140-6736(23)02409-1. PMID: 38245238.
-
Jackson DJ, Wechsler ME, Jackson DJ, Bernstein D, Korn S, Pfeffer PE, Chen R, Saito J, de Luíz Martinez G, Dymek L, Jacques L, Bird N, Schalkwijk S, Smith D, Howarth P, Pavord ID; SWIFT-1 and SWIFT-2 Investigators; SWIFT-1 Investigators; SWIFT-2 Investigators. Twice-Yearly Depemokimab in Severe Asthma with an Eosinophilic Phenotype. N Engl J Med. 2024 Dec 19;391(24):2337-2349. doi: 10.1056/NEJMoa2406673. Epub 2024 Sep 9. PMID: 39248309.
-
Kim LHY, Saleh C, Whalen-Browne A, O'Byrne PM, Chu DK. Triple vs Dual Inhaler Therapy and Asthma Outcomes in Moderate to Severe Asthma: A Systematic Review and Meta-analysis. JAMA. 2021 Jun 22;325(24):2466-2479. doi: 10.1001/jama.2021.7872. PMID: 34009257; PMCID: PMC8135065.
-
Kew KM, Dahri K. Long-acting muscarinic antagonists (LAMA) added to combination long-acting beta2-agonists and inhaled corticosteroids (LABA/ICS) versus LABA/ICS for adults with asthma. Cochrane Database Syst Rev. 2016 Jan 21;2016(1):CD011721. doi: 10.1002/14651858.CD011721.pub2. PMID: 26798035; PMCID: PMC9440477.















































